Antiseptic Surgery
by Joseph Lister
Introduction — the Englishman whose work belongs to Scotland
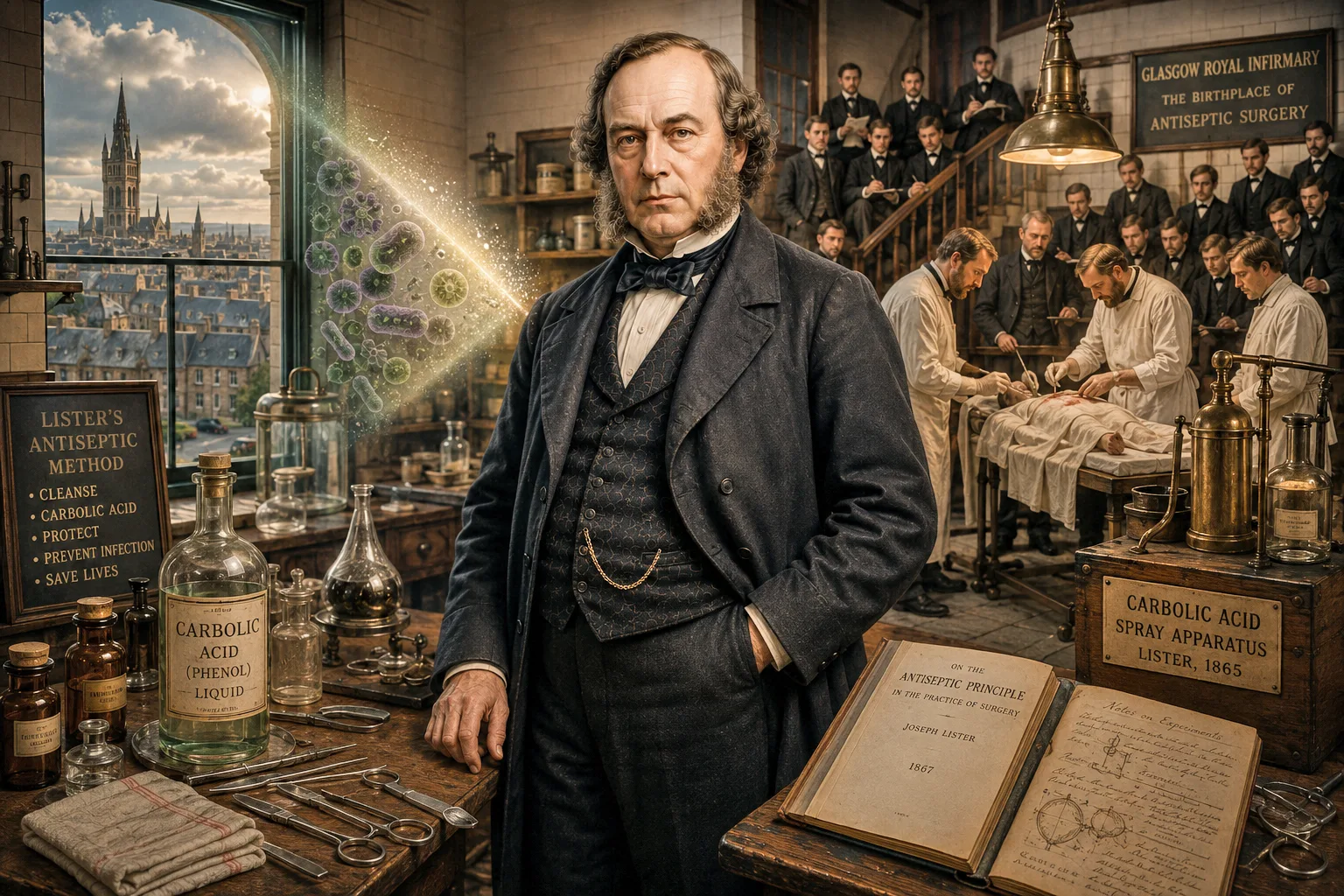
Joseph Lister was born in Essex and died in Kent. He was, by birth and burial, an Englishman. And yet the discovery that made him one of the most consequential figures in the history of medicine — the antiseptic principle that turned surgery from a near-certain death sentence into a safe and routine procedure — was conceived, tested and proven in Scotland. The first successful antiseptic operation in human history took place on 12 August 1865 at Glasgow Royal Infirmary. The eleven-year-old boy on the table, James Greenlees, walked out of hospital alive. Modern surgery walked out with him.
This is the story of how Joseph Lister, working as Regius Professor of Surgery at the University of Glasgow and later Professor of Clinical Surgery at the University of Edinburgh, took Louis Pasteur's germ theory out of the laboratory and into the operating theatre — and why every modern operation, from a routine appendectomy to a heart transplant, traces its lineage to a Glasgow ward in the summer of 1865.
The horror of pre-Lister surgery
Before Lister, an operation was a gamble with death. Anaesthesia, introduced by the Scot James Young Simpson with chloroform in 1847, had abolished the agony of surgery — but it had not made surgery safe. In the great Victorian hospitals of London, Paris, Vienna and Glasgow, between a third and a half of all major operations ended in the patient's death, not from the knife but from what came after: gangrene, erysipelas, pyaemia, septicaemia — the catch-all 'hospital diseases' that surgeons accepted as the unavoidable companion of their craft.
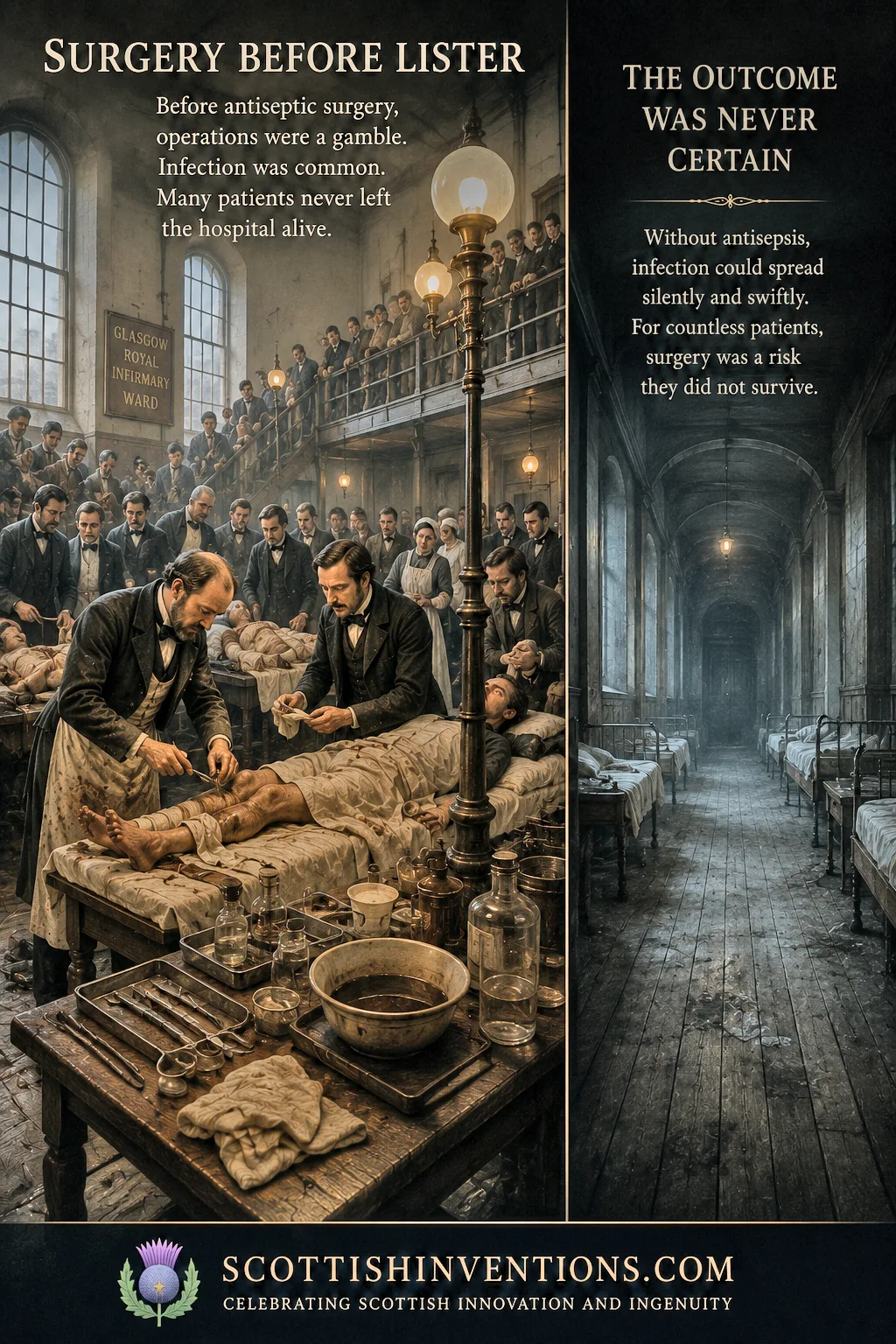
Surgeons operated in frock coats stiff with old blood, the lapels bearing dried pus as a badge of experience. Instruments were wiped on aprons between patients. Ligatures were held in the surgeon's mouth. Wards stank of putrefaction; the smell of laudable pus was held to be a sign that a wound was healing. At Glasgow Royal Infirmary, where Lister took up the Regius chair of Surgery in 1860, mortality after compound fractures and amputations sometimes ran above 60 per cent. Operating theatres, for all their dignity of name, were closer to charnel houses than to places of healing.
Nobody understood why. The dominant theory was 'miasma' — bad air, foul vapours from the wound itself. Some surgeons whispered about contagion. None had a workable answer. The honest ones, like the great Edinburgh surgeon James Syme — Lister's father-in-law and the most respected operator in Britain — confessed that they were powerless. Surgery had run, in the dread phrase of the day, into a wall of putrefaction.
Lister's road to Scotland — Edinburgh and Glasgow
Joseph Lister was born in Upton, Essex, on 5 April 1827 into a prosperous Quaker family. His father, Joseph Jackson Lister, was a wine merchant and a self-taught optical genius whose work on the achromatic microscope had revolutionised the study of cells. The young Lister grew up surrounded by microscopes — and with the Quaker conviction that science was, properly understood, a form of moral duty.
He took his medical degree at University College London in 1852 and, on the advice of his teachers, travelled north to Edinburgh to study under James Syme — the greatest clinical surgeon in the English-speaking world. He intended to stay a month. He stayed seven years. He became Syme's house surgeon, then his assistant, married his daughter Agnes Syme, was elected a Fellow of the Royal College of Surgeons of Edinburgh in 1855, and was appointed an extra-academical lecturer in surgery at the University of Edinburgh. Edinburgh made him a surgeon. Scotland made him a Scot in everything but birth.
In 1860 he was elected to the Regius Chair of Surgery at the University of Glasgow, with a parallel appointment as surgeon at Glasgow Royal Infirmary. He inherited the brand-new surgical wards of the Infirmary's Donaldson Building — and was appalled by what he found there. The mortality after his amputations was as bad as anywhere in Britain. He set himself, with characteristic Quaker doggedness, to find out why.
Pasteur's germ theory — the spark from France
The answer arrived from Paris. In 1864 a colleague at the University of Glasgow's chemistry department, Thomas Anderson, drew Lister's attention to the recent papers of the French chemist Louis Pasteur. Pasteur had shown that fermentation and putrefaction were not spontaneous chemical reactions in dead tissue, as had been universally assumed, but the work of living microscopic organisms carried in the air. Sterilise the air and the organisms, and decay stopped.
Lister read Pasteur in the original French, repeated his experiments at the bench in Glasgow, and saw at once what no other surgeon had seen: if Pasteur was right, then the suppuration that killed his patients was not a chemical inevitability but an infection — a biological attack on the wound by living microbes that could, in principle, be killed. The implications were almost too vast to bear. The surgeon's task was not merely to cut; it was to keep the wound free of the invisible enemy.
The next question was practical. With what could he kill the germs without killing the patient? Lister had read that the council of the Cumbrian town of Carlisle had successfully treated its sewage with carbolic acid — a coal-tar distillate that destroyed the stench and, it was suspected, the organisms that caused it. If carbolic could sterilise sewage, perhaps it could sterilise a wound.
The breakthrough at Glasgow Royal Infirmary (1865–1867)
On the afternoon of 12 August 1865, an eleven-year-old boy was brought into Ward 24 of Glasgow Royal Infirmary with a compound fracture of the left tibia. James Greenlees had been run over by the wheel of a cart in Glasgow's High Street. The bone had punctured the skin — and a compound fracture, in 1865, was as good as a death sentence. The conventional treatment was immediate amputation; even then, perhaps half of such patients died of infection within weeks.
Lister did something no surgeon had ever done. He cleaned the wound with carbolic acid. He wrapped it in lint soaked in carbolic. He covered the lint with tinfoil to prevent evaporation, splinted the leg, and left it. He changed the carbolic dressing at intervals. He waited.

James Greenlees — the boy who walked out of hospital
The wound did not suppurate. There was no gangrene, no fever, no blood-poisoning. After six weeks the bone had united cleanly. The boy walked out of Glasgow Royal Infirmary alive. Lister, with the caution of the scientist he was, treated ten more compound fractures over the next two years. Nine survived; the one who died was killed by a haemorrhage, not by infection. Before Lister, those eleven patients would, on the best Glasgow figures of the day, have produced six or seven corpses.
“Without you, gentlemen, I should have done nothing.”
Two years later, in March 1867, Lister published the case of James Greenlees and his successors in The Lancet under the title 'On a New Method of Treating Compound Fracture, Abscess, etc., with Observations on the Conditions of Suppuration'. A few months afterwards came the great theoretical paper, 'On the Antiseptic Principle in the Practice of Surgery'. Together they are the founding documents of modern surgery — and they were the report of work done not in London, not in Paris, not in Berlin, but in Glasgow.
In his Glasgow wards as a whole, Lister documented a fall in post-operative mortality from about 46 per cent in the years before he introduced antisepsis to about 15 per cent in the years after. No surgical reform before or since has produced such an improvement. It was, quite simply, the largest single saving of life in the recorded history of the operating theatre.
How antiseptic surgery worked — Pasteur's germ theory in Lister's hands
Lister's system rested on a single, almost philosophical insight: that the surgeon's enemy is invisible. If Pasteur's microbes caused putrefaction, then the wound had to be sealed against them. Lister achieved this in three layered ways. First, the wound itself was cleansed with a solution of carbolic acid. Second, all instruments, ligatures and dressings that came near it were soaked in carbolic. Third — and most controversially — the air above the operating field was filled with a fine carbolic spray, generated by a hand-pumped brass apparatus that became, for a generation, the symbol of Listerian surgery.
The carbolic spray was eventually abandoned (it poisoned the surgeons more reliably than the germs), but the principle survived intact. Sterilise the wound. Sterilise everything that touches the wound. Keep the microbes out, and the body's own astonishing capacity to heal will do the rest. In time the chemical antisepsis of carbolic gave way to the steam-sterilised, white-tiled, white-gowned asepsis of the twentieth-century operating theatre — but every gown, every glove, every autoclave is the lineal descendant of Lister's Glasgow ward.

How Lister's Antiseptic System Worked
Germs enter the wound
Lister accepted Pasteur's then-radical claim that microscopic organisms in the air, on instruments and on the surgeon's hands were the true cause of post-operative infection.
Infection begins
Without antisepsis, these microbes multiplied in the open wound, causing inflammation, suppuration, blood-poisoning and frequently death — the dreaded 'hospital diseases'.
Carbolic acid applied
Lister soaked dressings, instruments and ligatures in carbolic acid (phenol) and used a fine spray of carbolic in the air around the operating field.
Germs destroyed
Carbolic killed bacteria on contact, preventing them from colonising the wound. The principle was chemical antisepsis, the direct ancestor of modern surgical sterilisation.
Wound heals safely
With the wound shielded from putrefaction, tissue could knit cleanly. Lister could now operate on compound fractures and joints that had previously been a near-certain death sentence.
Patient survives
In Lister's Glasgow wards, post-operative mortality fell from about 46% to about 15% within a few years — the most dramatic improvement in surgical safety in history.
Return to Edinburgh — teaching a generation
In 1869, on the retirement of his old teacher and father-in-law James Syme, Lister was appointed Professor of Clinical Surgery at the University of Edinburgh and took charge of the surgical wards of the Royal Infirmary of Edinburgh. For eight extraordinary years he taught antiseptic surgery to crowded classes of medical students who came from every corner of the British Empire and beyond. Edinburgh, already the most famous medical school in the world, became the school of antiseptic surgery — and through its graduates, the methods born in Glasgow spread to every continent.
His Edinburgh students included some of the founding figures of modern surgery: Sir Hector Cameron, Sir William Macewen — who would become Lister's successor at Glasgow and the pioneer of brain surgery — and John Stewart, who carried Listerism to Canada. When in 1877 Lister finally accepted the Chair of Clinical Surgery at King's College London, he left behind in Scotland a doctrine, a method and an army of disciples. By the end of the 1880s, no respectable surgeon in the world operated without antisepsis. Lister had won.
Joseph Lister and Antiseptic Surgery — Key Dates
1860
Lister, already a Fellow of the Royal College of Surgeons of Edinburgh, is appointed Regius Professor of Surgery at the University of Glasgow.
1865
On 12 August at Glasgow Royal Infirmary, Lister performs the first successful antiseptic operation, dressing the compound leg fracture of 11-year-old James Greenlees with carbolic acid. The boy survives.
1867
Lister publishes 'On a New Method of Treating Compound Fracture, Abscess, etc.' and 'On the Antiseptic Principle in the Practice of Surgery' in The Lancet — the founding papers of modern surgery.
1869
Returns to Scotland's capital as Professor of Clinical Surgery at the University of Edinburgh, where his methods are refined and taught to a generation of surgeons.
1897
Created Baron Lister of Lyme Regis — the first British medical practitioner ever raised to the peerage, in recognition of his transformation of surgery.
1912
Lister dies on 10 February at Walmer, Kent. By this date antiseptic and aseptic surgery is standard practice in every modern hospital on earth.
Legacy — from Glasgow to every operating theatre on earth
Lister's legacy is the modern operating theatre itself. Every sterile field, every autoclaved instrument, every gloved hand and masked face, every drape of green cloth around the surgical site is the working out of the principle he established in Glasgow in 1865. The discipline of surgical asepsis, perfected at the end of the nineteenth century by surgeons like Bergmann in Berlin and Halsted in Baltimore, did not replace Lister's antisepsis: it grew directly from it.
His personal honours were unprecedented. He was created Baronet in 1883 and, in 1897, Baron Lister of Lyme Regis — the first British medical practitioner ever raised to the peerage. He served as President of the Royal Society from 1895 to 1900 and was a founder member of the Order of Merit on its creation in 1902. The Lister Institute of Preventive Medicine in London, the genus Listeria, the antiseptic mouthwash Listerine — all bear his name. The Lister Medal, awarded jointly by the four Royal Colleges of Surgeons, is among the most coveted prizes in world surgery.
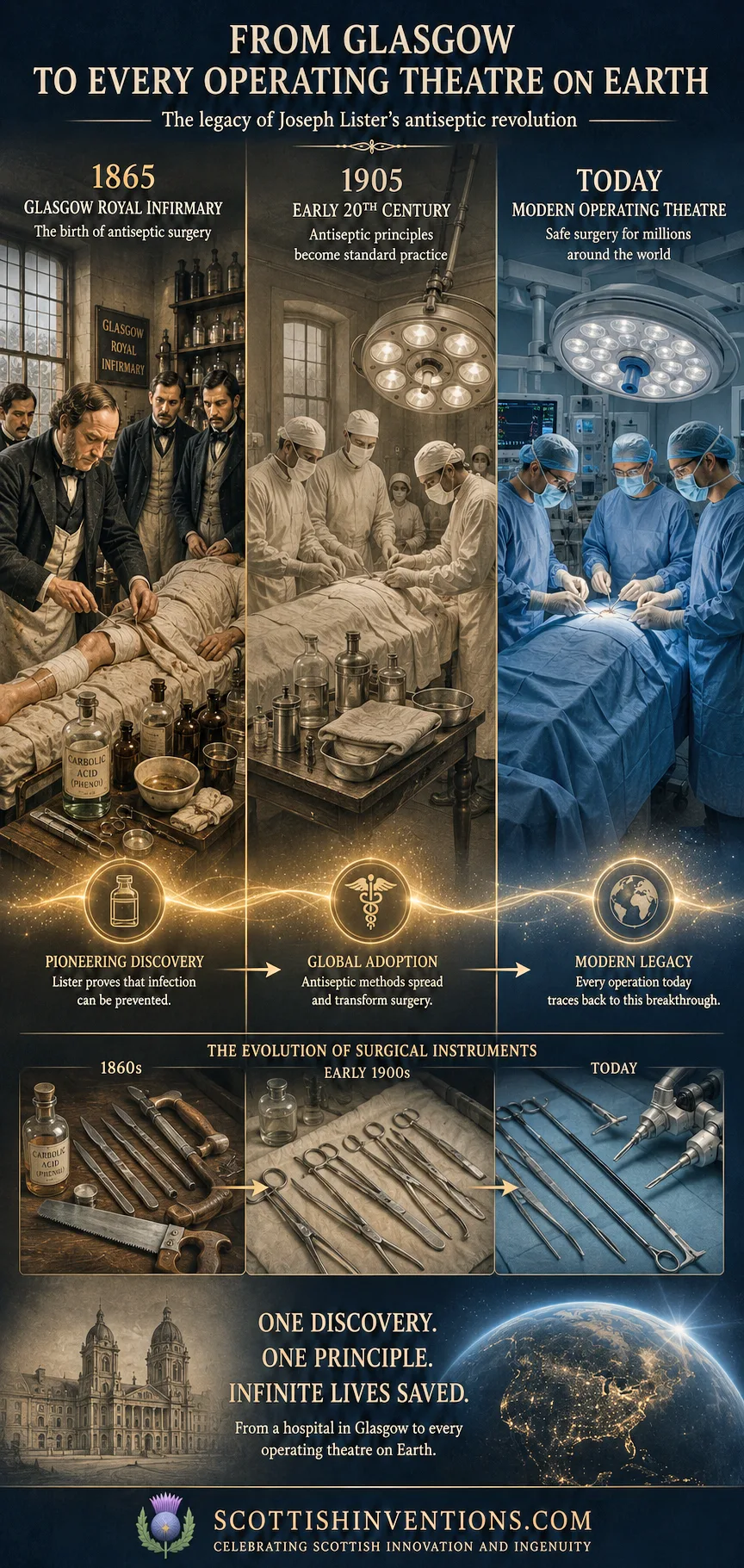
But the truest monument is statistical. Before 1865, perhaps a third to a half of all major surgical patients died of infection. Today, the post-operative infection rate in a modern hospital is well under one per cent. Every operation performed in the world today — there are more than 310 million of them every year — is performed under the sterile conditions that Joseph Lister, working at Glasgow Royal Infirmary, established. It is impossible to count the lives this has saved; the number certainly runs to the hundreds of millions, and may well run to the billions.
Conclusion — an Englishman, a Scottish discovery
Joseph Lister was English. The discovery that bears his name is Scottish. He carried it out at Glasgow Royal Infirmary and refined it at the University of Edinburgh; he was a Fellow of the Royal College of Surgeons of Edinburgh; his decisive papers were the report of Glasgow cases. To insist on this is not parochial. It is the simple historical truth that Scotland — through Glasgow's wards, Edinburgh's lecture theatres, and the Scottish medical tradition that taught Lister to think clinically and rigorously about what he saw — was the place where antiseptic surgery was born.
Scotland gave the world the steam engine of Watt, the telephone of Bell, the television of Baird, the modern economics of Smith, and the public service broadcasting of Reith. To that astonishing list belongs another gift, made jointly by a Quaker Englishman and the country that adopted him: safe surgery. From a Glasgow ward in August 1865 to every operating theatre on earth in the twenty-first century, the line is unbroken — and it begins with Joseph Lister and an eleven-year-old boy called James Greenlees.
Frequently Asked Questions
Was Joseph Lister Scottish? No — Lister was born in Upton, Essex, on 5 April 1827 and died in Walmer, Kent, on 10 February 1912. But almost the whole of his great work on antiseptic surgery was done in Scotland: as Regius Professor of Surgery at the University of Glasgow (1860–1869) and as Professor of Clinical Surgery at the University of Edinburgh (1869–1877). He was a Fellow of the Royal College of Surgeons of Edinburgh from 1855 and is widely regarded as one of the greatest figures in the Scottish medical tradition.
What was antiseptic surgery? Antiseptic surgery is the practice of preventing wound infection by killing the microbes that cause it. Lister, applying Pasteur's germ theory, used carbolic acid (phenol) to sterilise wounds, instruments, ligatures and dressings, and a carbolic spray to disinfect the air around the operating field. It is the direct ancestor of modern surgical asepsis — the sterile gowns, gloves, drapes and autoclaved instruments of every operating theatre today.
Who was James Greenlees? James Greenlees was an eleven-year-old Glasgow boy who, on 12 August 1865, became the first patient ever treated with antiseptic surgery. After being run over by a cart and suffering a compound fracture of the left tibia, he was admitted to Glasgow Royal Infirmary, where Lister dressed the wound with carbolic acid. He recovered without infection and walked out of hospital — the first survivor of modern surgery.
Why is Glasgow important in medical history? Because Glasgow Royal Infirmary is the birthplace of antiseptic surgery. It was in the Infirmary's surgical wards, between 1865 and 1867, that Joseph Lister carried out the first antiseptic operations and developed the system that transformed surgery worldwide. Glasgow's place in the history of medicine — alongside the University of Edinburgh's role in teaching the next generation of surgeons — is the reason Scotland is correctly described as the cradle of modern, safe surgery.
Related Inventions
Anaesthesia / Chloroform
James Young Simpson · 1847
Surgical anaesthesia using chloroform.
Watt Steam Engine
James Watt · 1769
The separate condenser that powered the Industrial Revolution.

Weekly Scottish Innovation Facts
Delivered to your inbox every Sunday. No spam, just brilliance.