Glasgow Coma Scale
by Graham Teasdale & Bryan Jennett
Introduction — a Scottish hospital that changed medicine
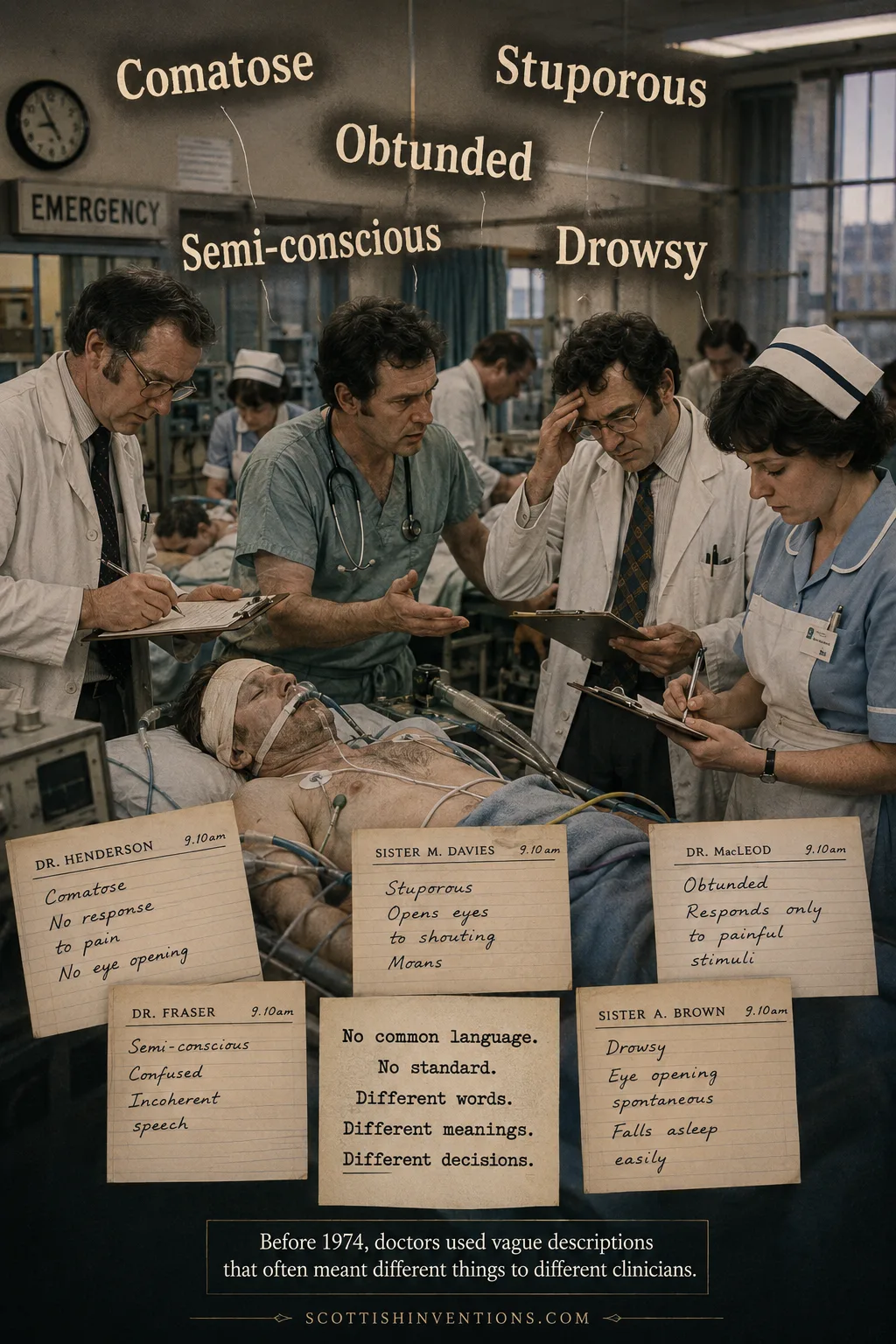
The Glasgow Coma Scale is arguably the single most influential clinical tool ever to come out of a Scottish hospital. Invented in 1974 by two neurosurgeons working in Glasgow's Institute of Neurological Sciences, it replaced a confusing babble of vague words — 'stuporous', 'obtunded', 'semi-conscious', 'drowsy' — with a clear, numbered scale that any nurse, paramedic or doctor on Earth can apply in under a minute.
Half a century on, it is still in daily use, essentially unchanged, in ambulances, emergency departments and intensive care units across the planet. The original Lancet paper is among the most-cited in the history of clinical medicine. This is the story of how Graham Teasdale and Bryan Jennett — both English-born, both Glasgow-based — quietly built a tool that now saves lives in more than 80 countries, every hour of every day.
The Problem — Why a Coma Scale Was Needed
Before 1974, assessing an unconscious patient was an exercise in linguistic guesswork. One doctor's 'stuporous' was another's 'obtunded'; a third would write 'semi-conscious', a fourth 'drowsy'. Words shifted meaning between wards, between hospitals, and between night and day shifts. A patient who had been 'comatose' at midnight might be 'semi-conscious' by morning — not because anything had changed, but because a different clinician had reached for a different word.
For head-injured patients the cost of this vagueness was measured in lives. Subtle deterioration — the first sign of a brain bleed, of rising intracranial pressure, of an injury demanding urgent surgery — was easy to miss when each handover used its own private vocabulary. Glasgow's Institute of Neurological Sciences, where Teasdale and Jennett worked, was one of the busiest head-injury units in Britain, and they saw the cost of the linguistic confusion every week.
The Inventors — Two Englishmen in Glasgow
Sir Graham Teasdale was born on 23 September 1940 in County Durham, England. He qualified in medicine at the University of Durham — at the medical school in Newcastle upon Tyne — graduating MB BS in 1963. After junior posts in Newcastle, London and Birmingham, he arrived in Glasgow in 1967, first as a lecturer in Anatomy at the University of Glasgow and then as a neurosurgical trainee at the Southern General Hospital. When the Glasgow Coma Scale was published in 1974 he was a neurosurgical senior registrar; he rose to Professor and Head of the University of Glasgow's Department of Neurosurgery from 1981 to 2003.
Bryan Jennett was born in Twickenham, west London, in 1926. He trained in medicine at the University of Liverpool and, after fellowships in the United States, was appointed Professor of Neurosurgery at the University of Glasgow in 1968. There he founded the Institute of Neurological Sciences at the Southern General Hospital in Govan — a deliberately integrated centre that brought neurosurgeons, neurologists, neuroradiologists and rehabilitation specialists onto a single site. It was in that institute that the work on coma scoring would be done.
Neither was a born Scot. Both did their defining work entirely in Scotland. The Glasgow Coma Scale belongs to Glasgow in the same way that antiseptic surgery belongs to Glasgow through Joseph Lister, or obstetric ultrasound through Ian Donald — by virtue of the city's wards, its laboratories, and the Scottish medical tradition that adopted them.
The Invention of the Glasgow Coma Scale (1974)
Teasdale and Jennett's insight was deceptively simple. Instead of trying to capture 'level of consciousness' in a single word, they would break it into three independent observations — each of which any trained clinician could make reliably at the bedside — and then sum them into a single number.
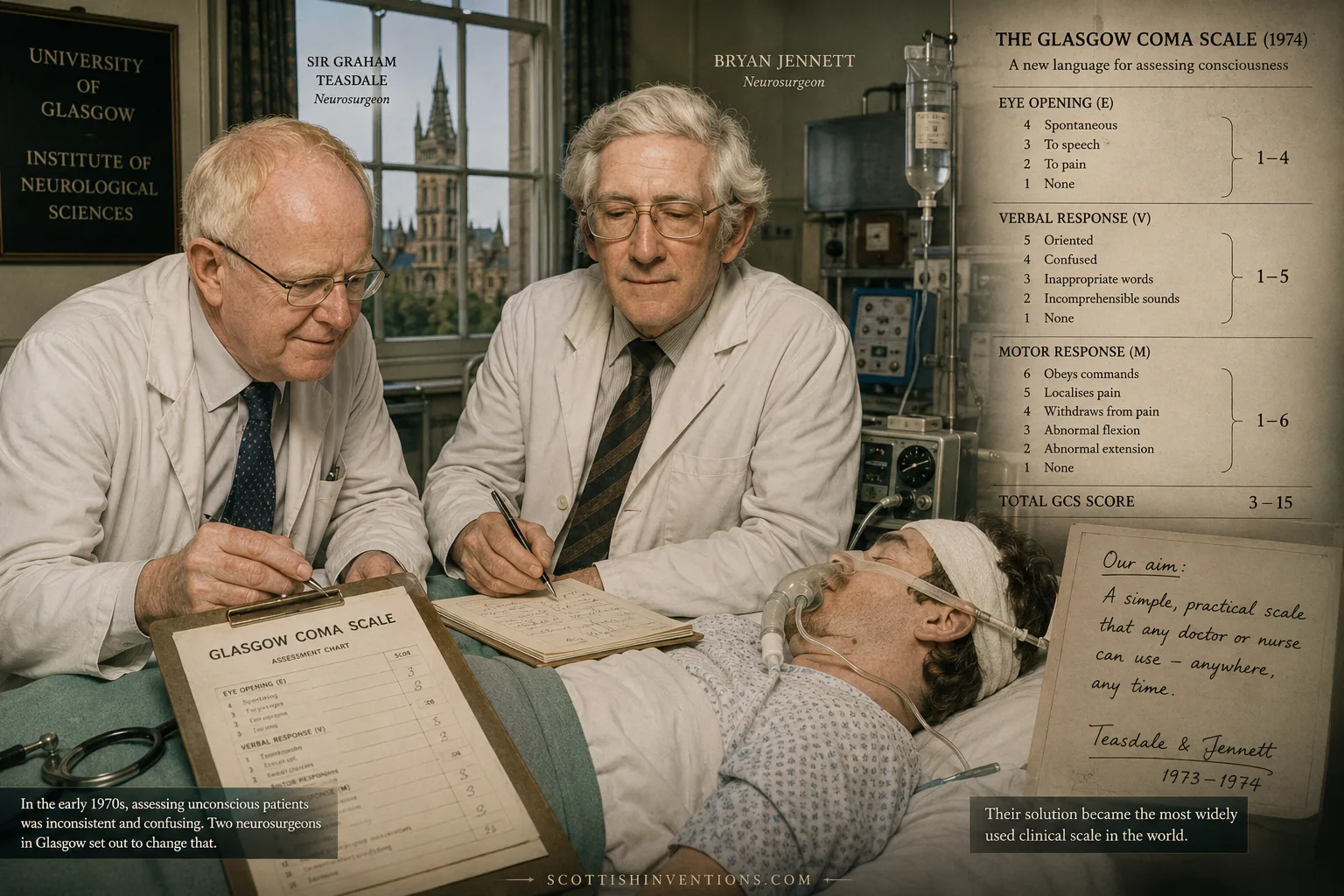
They chose Eye opening (scored 1 to 4), best Verbal response (1 to 5) and best Motor response (1 to 6). Each category was anchored to concrete, observable behaviours: not 'drowsy' but 'eyes open to speech'; not 'confused' but 'oriented to person, place and time'; not 'responsive' but 'localises pain'. The scores were summed to give a total from 3 (deep coma, no response at all) to 15 (fully alert). Crucially, the component scores were as important as the sum — 'E3 V4 M5 = 12' tells a story that 'GCS 12' alone cannot.
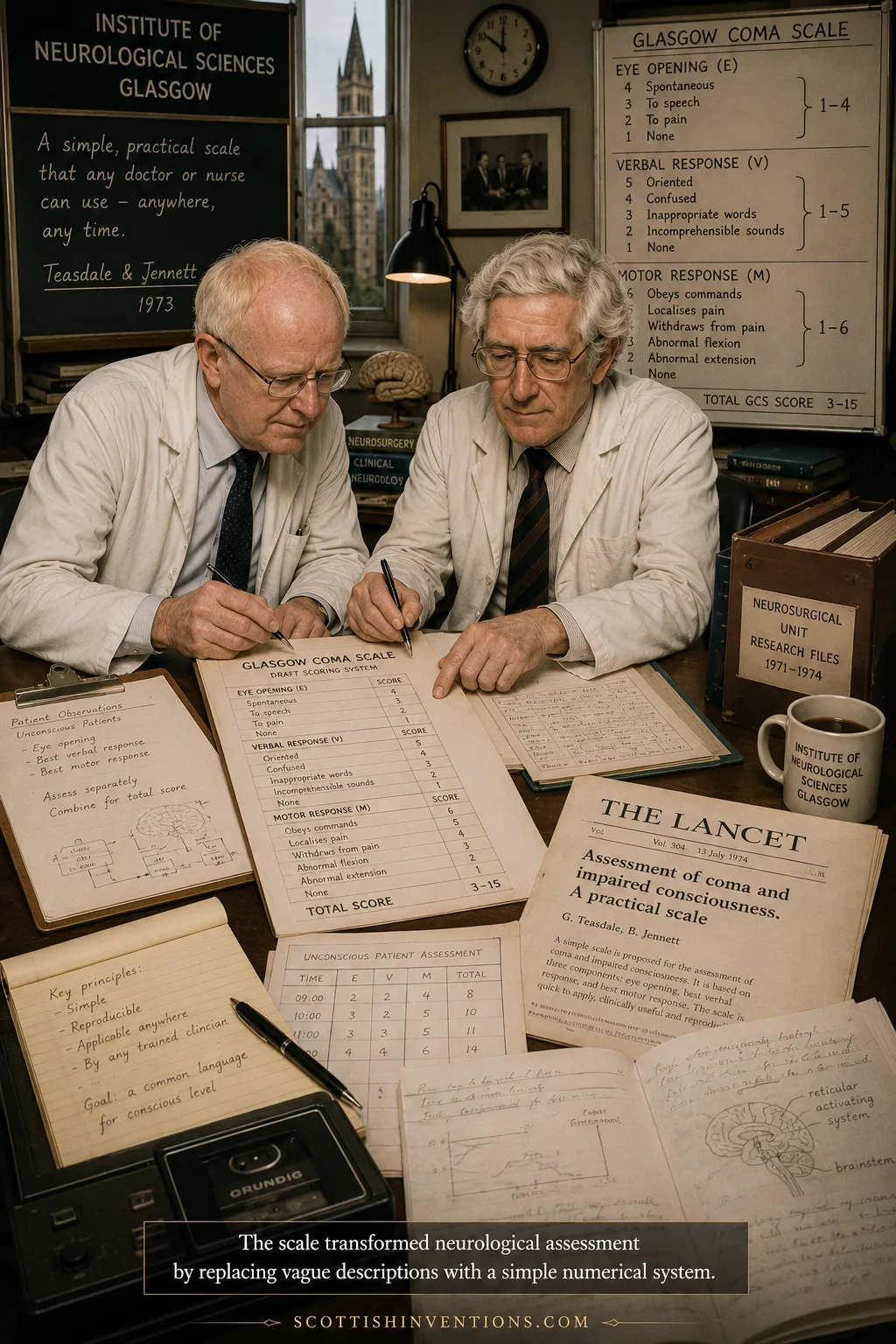
Their paper, 'Assessment of coma and impaired consciousness. A practical scale', appeared in The Lancet on 13 July 1974. It is barely four pages long. It contains no statistics more complex than a percentage. And it has become one of the most-cited papers in the history of clinical medicine, with tens of thousands of citations and a measurable influence on the survival of head-injured patients in every country on Earth.
The Glasgow Coma Scale — Key Dates
1967
Graham Teasdale arrives in Glasgow as a lecturer in Anatomy at the University of Glasgow, before entering neurosurgical training.
1968
Bryan Jennett is appointed Professor of Neurosurgery at Glasgow, founding the city's Institute of Neurological Sciences at the Southern General Hospital.
1973
Teasdale and Jennett begin systematic work on a structured, reproducible bedside scale to replace the vague vocabulary then in use.
1974
On 13 July, 'Assessment of coma and impaired consciousness. A practical scale' is published in The Lancet — the founding paper of the Glasgow Coma Scale.
1977
Teasdale and Jennett publish the Glasgow Outcome Scale, the companion tool for grading recovery after brain injury.
2008
Bryan Jennett dies in Glasgow on 26 January, aged 82, by then recognised as one of the founding figures of modern neurosurgery.
How the Scale Works
The Glasgow Coma Scale is built around three independent responses, scored separately and added together. Eye opening runs from 4 (spontaneous) to 1 (none). Verbal response runs from 5 (oriented) to 1 (none). Motor response runs from 6 (obeys commands) to 1 (none). The total runs from 3 to 15.
A score of 13–15 indicates a mild brain injury; 9–12 moderate; 3–8 severe. A GCS of 8 or below has, for decades, been the conventional threshold for considering airway protection in head injury. Crucially, the scale is meant to be repeated — every few minutes in an ambulance, every few hours in an intensive care bed — because the trend matters as much as any single reading.

How the Glasgow Coma Scale Works
Eye Opening (E) — 1 to 4
Scored from 4 (spontaneous) down through 3 (to speech) and 2 (to pain) to 1 (no eye opening at all).
Verbal Response (V) — 1 to 5
Scored from 5 (oriented to person, place and time) through 4 (confused), 3 (inappropriate words), 2 (incomprehensible sounds) to 1 (no verbal response).
Motor Response (M) — 1 to 6
Scored from 6 (obeys commands) through 5 (localises pain), 4 (withdraws), 3 (abnormal flexion / decorticate), 2 (abnormal extension / decerebrate) to 1 (no movement).
Total GCS = E + V + M
The three component scores are summed for a total between 3 and 15. The component scores matter as much as the total — 'E3 V4 M5 = 12' is more informative than just '12'.
Clinical thresholds
13–15 mild brain injury; 9–12 moderate; 3–8 severe. A score of 8 or below has, for decades, been the conventional indication to consider intubation in head injury.
Repeat, repeat, repeat
The scale is designed to be applied serially — every few minutes in an emergency, every few hours in intensive care — so that any deterioration in consciousness is caught early.
Legacy
Half a century on, the Glasgow Coma Scale is part of the basic clinical vocabulary of medicine. It is taught in every medical and nursing school on Earth, written into the trauma protocols of more than 80 countries, and printed on the front page of ambulance run-sheets from Glasgow to Tokyo to São Paulo. The companion Glasgow Outcome Scale, published by Teasdale and Jennett in 1977, plays the same role at the other end of the journey — grading how well a brain-injured patient eventually recovers.
Bryan Jennett died in Glasgow on 26 January 2008, aged 82, by then recognised as one of the founding figures of modern neurosurgery. Graham Teasdale was knighted in the 2006 New Year Honours and continues to update and steward the scale through the official Glasgow Coma Scale website hosted by the University of Glasgow. Both men were elected Fellows of the Royal Society of Edinburgh.

From a Glasgow ward to every hospital on Earth, the Glasgow Coma Scale is a quiet Scottish gift to medicine — proof that the most transformative clinical tools are not always the most technologically dazzling, but the ones simple enough that anyone can use them, anywhere, any time.
Frequently Asked Questions
Who invented the Glasgow Coma Scale? The Glasgow Coma Scale was invented in 1974 by Graham Teasdale and Bryan Jennett, two neurosurgeons working at the Institute of Neurological Sciences at the Southern General Hospital in Glasgow. Their paper, 'Assessment of coma and impaired consciousness. A practical scale', was published in The Lancet on 13 July 1974.
Were Teasdale and Jennett Scottish? No — both were English-born. Sir Graham Teasdale was born in County Durham in 1940; Bryan Jennett in Twickenham in 1926. But both did their defining work entirely at the University of Glasgow, where the Glasgow Coma Scale was conceived, tested and proven. The scale is a Scottish invention by virtue of the city, the institution and the medical tradition in which it was created.
How does the Glasgow Coma Scale work? The GCS scores three independent responses — Eye opening (1–4), Verbal response (1–5) and Motor response (1–6) — and sums them to a total between 3 (deep coma) and 15 (fully alert). A score of 13–15 indicates mild brain injury, 9–12 moderate, and 3–8 severe.
Why is the Glasgow Coma Scale important? Because it gave clinicians worldwide a common, reproducible language for assessing consciousness. Before the GCS, doctors used vague, overlapping words like 'stuporous' and 'obtunded' that meant different things to different people. The scale is now used in more than 80 countries, taught in every medical school on Earth, and embedded in trauma and intensive-care protocols globally.
Related Inventions

Anaesthesia / Chloroform
James Young Simpson · 1847
Surgical anaesthesia using chloroform.

Weekly Scottish Innovation Facts
Delivered to your inbox every Sunday. No spam, just brilliance.